This will be the first in a series of posts on the sessions I attended at CSM 2017 in San Antonio, Texas. I, as one individual, could no way have attended ALL of the 300+ educational sessions available at CSM, nor were all 300+ applicable to my personal interests. In fact, some of the sessions I did attend are not terribly applicable to the interests here in the blog. So I’ll just cover applicable items. I strongly encourage every physical therapist in the audience to attend CSM or the NEXT conference at some point in the near future. NEXT is happening this summer in Boston and CSM for 2018 will be in New Orleans.
~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
The first session I attended on Thursday was on Pusher Syndrome by Vicky Prado and Suljay Galen.
First, what is Pusher Syndrome and how does it present? This is what you’ll see clinically in a brain injured individual including stroke that has Pusher Syndrome:
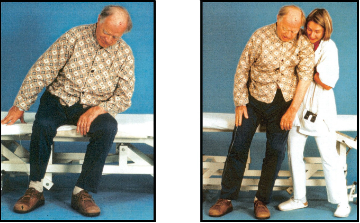
— Pushing towards involved side
— Poor awareness of where their own midline is located
— Strong extension and abduction of the uninvolved side
— Resistance to external correction toward midline
All of the above MUST be present in some position/activity. I’ve had people not really show it to me until I have them stand and walk. Others I could see it when I walked in their hospital room, because they were curled up one side of their bed it was so severe.
Some times this condition comes with a hemi visual neglect or poor sensation on the involved side as well. This doesn’t occur in all cases however.
Pusher Syndrome needs to be differentiated from thalamic astaisa, Wallenburg’s Syndrome, and vestibular cortex stroke, which is most easily done clinically by visualization of active pushing, which is not present in the others.
One of the reasons it is SO difficult to find any guidance in treating these folk is that no one has agreed on what to call this phenomenon, so looking it up by one term may not get you what you want. This clinical picture can be called:
— Pusher Syndrome (not generally in the literature)
— Contraversive pushing (This is what I call it in my documentation, as this is the term I’ve seen most commonly used in the literature.)
— Ipsilateral Pushing (Second most common term I’ve seen.)
— Unilateral neglect syndrome (To me this is a smaller category of people than a plain Pusher, as described above)
— Lateropulsion
The neuologic pathophysiology in play here fascinates me. As always, the 3 most important rules of brain pathology are: location, location, location. The problem areas seem to be slightly different depending on the side involved. For left brain it’s the anterior insular cortex, the operculum, the internal capsule and lateral thalamus. For the right brain it’s the posterior insula, superior temporal gyrus, operculum. What does that mean? These are deep brain structures mostly that are largely association areas of somatosensory and vestibular senses. So the basic problem here is that the visual and vestibular input these people are getting aren’t lining up correctly. They can’t feel where their bodies are is relation to gravity. I also found it interesting that actual sensation– touch– has nothing to do with Pusher Syndrome. It’s all visual and vestibular!
The literature is scant and not very helpful for treatment ideas on this population. What we do know is:
— Pusher Syndrome greatly slows recovery
— more useful to think of it as a motor or graviceptive (sense of gravity) neglect vs. a visual neglect
— that the problem is not purely visual nor purely vestibular, so targeting those two areas for treatment individually does not help, but keep in mind using them individually as compensatory measures
— visual and postural vertical don’t match up, so the pushing behavior is the patient’s attempt to correct for that as they feel their center of mass is too far to the uninvolved side.
— midline shifts in a hemorrhage does NOT make for Pusher Syndrome
— for many (62% in one study) the symptoms are resolved in 6 weeks, but for some they persist and are still present at 6 months (21%)
— 3 sources of deficits can be present in Pusher Syndrome: motor, proprioceptive and visio-spatial
To assess these folks there are 2 scales: the Clinical Scale for Contraversive Pushing (this is the one I had been using. Very clinic friendly, but not really useful as an outcome measure.) and the Burke Lateropulsion Scale (more time consuming, but looks to be more responsive to small changes, so more useful as an outcome measure and with research in my opinion. Click the link to download the article. Then the instructions for the tool are at the bottom of the article.)
Now the fun part: treatment. What do we do with these often very challenging people?! Here are a few ideas from the presentors and also some experienced clinicians that came to the mic after the presentation.
— Lokomat or other robot assisted gait training devices
— computer generated interactive visual feedback training (I honestly don’t know what this looks like. Anyone else? From Yang, et. al in 2014 if you’re curious.)
— mirror visual feedback training
— allow patient (in safe environment) to repeatedly experience the consequences (falling over) of his self-generated loss of balance so that they can recognize that their perception of upright is not accurate. Then ask them to find a way to get upright again. Assist if necessary.
— use tactile and verbal cuing to orient patient to true vertical less visual cues says one method. Have them close their eyes and feel where their body is in space, then cue them to put more of their weight to the left/right, etc.
— 0ther methods (including my own) find visual cues helpful. Draw attention to other objects in the environment that are upright. I like to use door frames or other structural references for this as most anyone will agree with you that structures are vertical, even the demented or cognitively involved ones.
— a focus on recognizing midline and weight shifting
— give them something to do actively with the pushing side so that they aren’t actively pushing so much. If their arm is really involved, I’ll tell them their main job is to take care of the hemiparetic arm and make sure it doesn’t get lost in transfers or fall down when they’re sitting or standing. Or if that doesn’t work, I’ll just give them something that I insist is of vital importance that they hold for me, like a roll of tape or a towel. With the leg, I’ll ask them to keep time with the music in the gym or to march with it to the beat or something like that.
— when they can align well with cuing, start removing your cues and then advance to maintaining vertical while distracted with conversation or playing a table top game like dominos, connect four, cards, etc.
— consider using a pelvic seat belt when seated in early phases
— do a lot of reaching activities, particularly toward the uninvolved side
— emphasize sit to stand training over transfer training
— body weight supported treadmill training
— instead of standing in parallel bars, stand with light touch next to mat
— put pushing leg on step or brick to decrease pushing lever
— put a slippery surface under hand, like a Frisbee, to again decrease pushing
— put a messenger bag with weight in it over uninvolved shoulder or have them carry a suitcase on uninvolved side to increase weight shift in standing
— don’t forget to strengthen the weak side!
— group treatment ideas for these folk could be seated balance, supine weight shifting and bed mobility activities
— train the family early on to do treatment with the involved side outside therapy time, so that your treatment sessions can focus more on the postural vertical which is the more immediate problem
— use a rolling table on the uninvolved side during gait training
— start standing on the tilt table, standing frame, in the water or in Arjou walker
— first goal: be able to maintain side bending to uninvolved side to where on elbow for 30 seconds
— put a tilt board under pelvis to increase awareness of tilt
— try doing activities in tall kneeling as a step between sitting and standing activities. To get into tall kneeling on a mat, stand facing the mat and then kneel on the edge with feet hanging off the edge.
That’s what is available in the literature at the moment and the suggestions of the clinicians at the mic. Vicky has an article currently under review for publication in the Journal of Neurologic Physical Therapy on Pusher Syndrome. I eagerly await it’s arrival in my mailbox, and so I won’t steal her thunder on her research, but it’s AWESOME and takes all the above and makes a treatment plan. So keep your eyes peeled, because I will definitely highlight it here on the blog when it comes out.

{kind=link}
Hi Bria,
I would like to thank you for posting above, really interesting.
So I’m Simon, currently studying Physical Therapy in Amsterdam, The Netherlands. I’m writing an bachelor thesis at the moment, concerning “the Pusher-Syndrome” and i’m interested in the article written by Vicky. Do you have any knowledge when it will be published and do you have any information about the design of the study/article/research
Sincerely,
Simon
LikeLike
Hi Simon! At the time of the conference, there was not a set date for the publication of Vicky’s article. She said it was under review at the time. It will be coming out in the Journal of Neurologic Physical Therapy. They may know a better time frame, depending on where in the review process the article is exactly. As for the design, it’s a case study series of 5 subjects with Pusher Syndrome in which Vicky applies her treatment strategies and documents before/after treatment outcomes. Good luck with your thesis!
LikeLike